


Networks and How to Better Apply Them To Mental Health

Introduction to Networks
I don’t study networks or know much about them. But I like to pretend to. Will you pretend with me?

I imagine the idea of networks is that they occur whenever there are a collection of things working together. I don’t remember where but I feel like I’ve heard these “things” are called nodes. So these nodes interact/connect with other nodes around them. And whenever there’s a whole lot of these connections, then the whole node-connection-thingy-ma-jigger creates something BIGGER than sum of the nodes themselves. It’s a magical thing, really.
I’m told the brain is a network. Here’s a visual I made.

See how the connections make a nice shape, a star! The star occurs when the things are working optimally. The star is the magical thing I was talking about- the property bigger than the nodes themselves!
If each node is equal to 1, this network would create something like 1+1+1+1+1 > 5. I don’t remember math working this way in school, but somehow it just makes sense to me when we’re discussing networks.
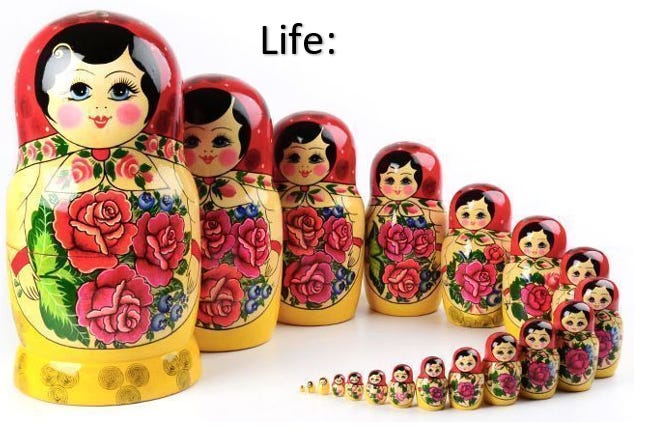
What’s crazy about life is that it’s networks out of networks… out of networks… out of networks, etc, etc, etc.
Atomic networks make molecules, molecular networks make macro-molecules (f.e. proteins), which make organelles, which make cells, which make organs, which make people, which make families, which make societies, which make…
Each network is just the star of the nodes (but also so much more). The complexity of something as superbly magical as life can only be understood as an Infinite-Russian-Nesting-Doll creating magical stars out of magical stars out of magical stars.
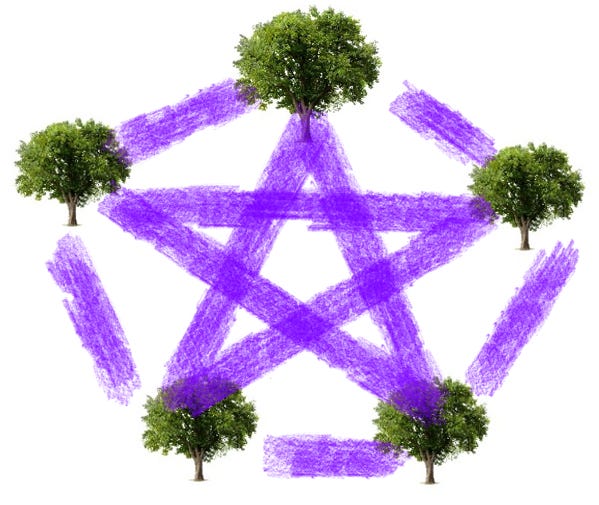
Does this make sense? I know you already know all this network stuff. You’ve said the phrase “Missing the forest for the trees” right? That’s proof that you get it. Trees are just the nodes of the forest. If I were to re-phrase the saying, I could say: “Missing the magic for the nodes”. Or I could draw the phrase:
When Networks Become Dysfunctional
Mental health treatment can be looked at through the lens of attempting to fix/optimize dysfunctional networks.
Let’s look at a specific example of using medication to treat mental illness. The theory behind drug treatment in network terms goes something like this:
there is a problem in a network…
the problem causes dysfunction across the network…
the dysfunction causes the network to lose its star (magical properties)…
the loss of the star means sub-optimal functioning…
this leads to symptoms...
treatment fixes the network…
the star returns…
the symptoms go away…

I could call the network above the Network-that-when-not-working-causes-depression. So if a doctor talks to a patient and thinks they’re depressed, then they’ll visualize the person’s network as the picture on the right. It’s easy to see that in this dysfunctional network, the star is gone. Which means that the magical emergent-properties that amounts to “not-depressed” isn’t there. The math here if each node equaled 1 would be something like 1+1+1+1+1<5.
So in depression how do we fix it? We just need some purple chalk.
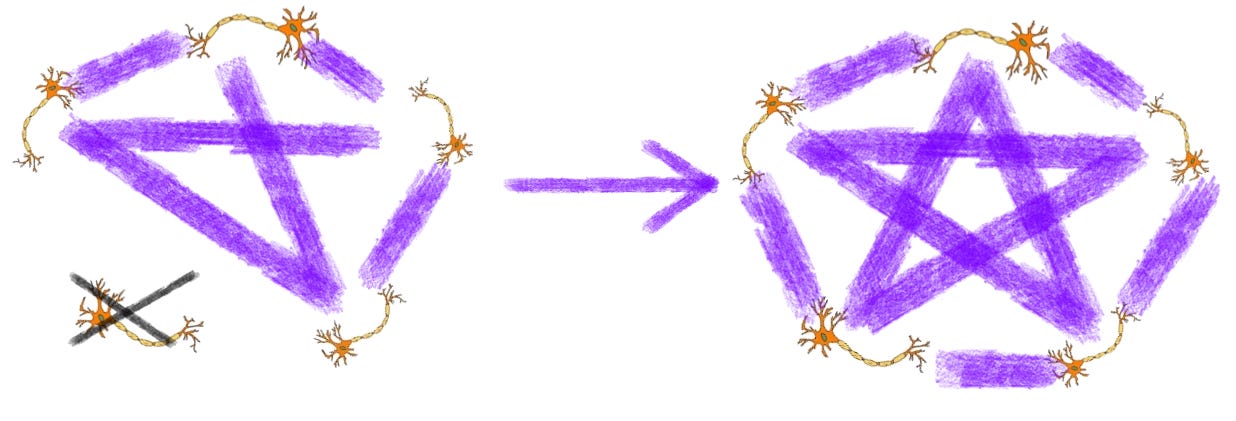
One of the key proteins that is increased when someone recovers from depression is BDNF. Now that we know how important networks are, it should be no surprise that BDNF is literally a connection maker... it’s involved in synaptic plasticity (synaptic = fancy-neuron-word for connection, plasticity = fancy-neuron-word for maker). So we can think of BDNF as the purple chalk that restores this network1.
When Models Become Dysfunctional
One model of mental illness is based on monoamines and their deficiencies

As you can see the model is far too simplistic. In fact, it’s so simplistic that it doesn’t even build a star. Just a lowly triangle. Sadly, a lot of people still base their treatment decisions entirely on this model2. They’ll say things like “well it’s more complex than this”… and then base their entire treatment algorithm on it anyway.
The pipedream in psychiatry is that one day we’ll know all the important neural-networks. And then some sort of brain-network-genetic-imaging-test will be able to identify which network is dysfunctional in a person…. And we’ll be able to use a treatment specific for fixing that network… And the wonderful star will return! A lot of people really want this to be the case. It would make all that time studying brain-stuff worth it. The truth is though, we just don’t know enough for this to be anywhere near how things work today.

This is a rat model of the depression-network. The acronyms are different areas of the brain, and make up the nodes of a hypothesized “depression network”. Since this is a rat model, we know humans are way MORE complicated than this. Already today some smart people know what all these acronyms stand for, and can speak very intelligently about how the mPFC has connections with VTA which synapses on the NAc, etc, etc, etc. But at the end of the day, behind the curtain, 99% of psychiatric decision-making is based on the lowly triangle.

So even though we can’t fix people based off our understanding of the neural-networks of the future (even if we really want to or even if we pretend that we are), I still think mental health providers need to pay close attention to networks. Actually, if I had to define the problem of mental health today… I would say that we’re hyper-focused on a single network that we don’t really understand (a neurobiological one), and don’t pay any attention to the networks that we do understand…
A Good Model Used Incorrectly Becomes Dysfunctional
Today the biopsychosocial model is taught widely across medical and psychiatric training. The gist of this model can be accurately deduced from the name: disease (e.g. mental-health) is the result of biological, psychological, and socio-environmental factors.

This model also has a “behind the curtain” truth to how it’s used in practice. The main paradigm today doesn’t view mental-health as the intersection point of biology, psychology, and sociology (as seen in the visual above). Rather, the main paradigm today views mental-health as psychosocial factors and sociological factors modulating what is ultimately a biological phenomenon (as seen in the visual below).

So the vast majority of biopsychosocial formulations today look something like: Patient has Generalized Anxiety Disorder, exacerbated by X-Y-Z psychosocial stressors. The implication here is that there is a primary problem with the person’s neurobiology (their Generalized-Anxiety-Disorder-circuits), and psychological/social factors are influencing it in some vague way.
The problem with using the word “factor” (definition per Webster: “something that helps produce or influence a result”) is that psychological/social dysfunction don’t just help or influence the problem in a person’s mental health…. often it’s the case that psychological/social dysfunction is the problem.

So behind the Curtain, the biopsychosocial model is practiced as the Biological Model with Psychosocial Factors. And the formulation becomes the plan: Patient has Generalized Anxiety Disorder, exacerbated by X-Y-Z……. start Zoloft. Starting Zoloft isn’t necessarily the wrong answer. But if it’s started under the biological model, the doctor should say: “This will treat your problem”. If it’s started under the biopsychosocial model, the doctor should say “This will help you so that you can start working on your problem”. It’s a subtle but important difference.
So to recap: the problem with the biological approach (often masquerading as the biopsychosocial model) is that the majority of mental health problems are not primary neurobiological problems. And this is central to where we’re going next: if a certain mental-health-diagnosis results in an identifiable issue at a neurobiological network, that doesn’t imply that the core deficit is a neurobiological one.
This is where I think networks can better capture what is going on with “mental health”.
A Better Model, Based on Networks We Do Understand
Mental health can be understood as the result of tightly inter-connected networks… networks that are highly influenced by their nodes and meta-stars.
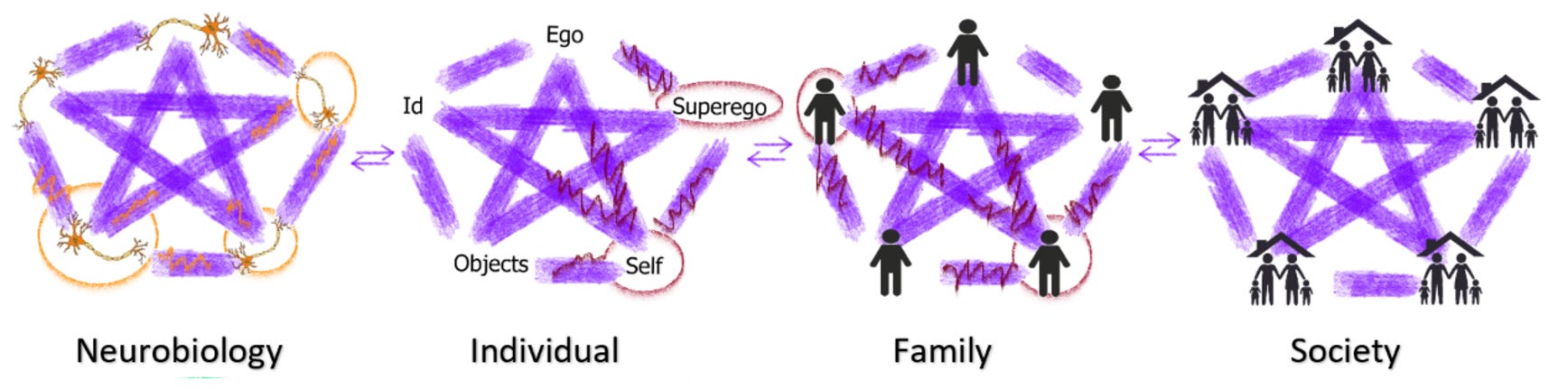
Here is a crude representation of a network/meta-network model3.

Symptoms of mental illness can develop through dysfunction in any of these network. When I look at this model, it looks very similar to the bio-psycho-social model. But by moving from “factors” and into “networks”, there are 2 key advantages.
1) Networks more intuitively capture the influence each network plays on the other networks. The node / star / 1+1+1+1+1 > 5 stuff captures how the neurobiology creates the individual, but the individual is more than the neurobiology. Which means the individual level should be its own object of study/treatment, completely independent of the neurobiological level (even though it’s created by it). A good metaphor here is physics > chemistry > biology. Biology is just made up of chemistry, which is made up of physics. But to master the different subjects requires completely different skill-sets. Newton would have never cracked evolution, Darwin would have never figured out gravity. That is to say: a psychopharmacologist can’t cure a family problem… a therapist can’t cure an acute manic episode.
2) it fixes the “factor” problem in how bio-psycho-social model is used today (the implicit assumption being that there are psychological/social factors that contribute to a biological disease). Networks better capture that the problem in the psychological or social networks can be the pathology in and of itself.
And to best visualize how these things influence one another, I will add one last visual-metaphor. Mental health is a fountain, each network a rung, crucial for the fountain to flow properly.

Now we can see that if there is a significant dysfunction at one level, it will cause issues downstream at the others levels. And that it is impossible to fix the core pathology by working at the wrong level4. So if there is a core dysfunction at the family level, the problem will flow to the individual and neurobiological level. But if you attempt to “fix” the neurobiological network dysfunction (medicate the person) without addressing the core dysfunction (family network dysfunction), then you’ll continue to see problems in that person’s life.
Children are increasingly being given the diagnosis of depression/ADHD/anxiety. These are umbrella categories with near infinite causes. When they’re pitched as “biological” or “neurological”, they do a huge disservice to the true complexity of what is going on. I’m not suggesting biological depression and biological ADHD don’t exist, but that primary biological depression/ADHD are exceedingly rare. The vast majority of symptoms of depression/anxiety/ADHD in children are deficits in the family network… that then trickle down to deficits in the individual, that trickle down to the neurobiological network. The individual and the neurobiology become problems in their own right, which require treatment. But the fountain won’t flow effectively until the you address the bottle-neck caused by the family-network dysfunction.
An example is a neglected child with abusive parents manifesting symptoms of ADHD, who is acting out in school. Look at how wildly different the formulations look for this neglected child with ADHD:
In a neurobiological formulation: the child has a neurobiological deficit, with psychosocial stressor of his home life. He is acting-out because of poor executive function, a manifestation of his dysfunctional brain circuits. The plan communicated to the family: “Stimulants will fix his brain, as the problem is in the child’s brain”.
In a network formulation: the child has significant dysfunction in his family network. He has no words to express that the people who are supposed to protect him are neglecting him (to a child, attention is the most important currency; a hug is preferred, but a beating will do). Acting out serves a very important individual function: getting attention. The plan communicated to the family: “Stimulants will help to minimize problems in the child’s school life while family therapy is done, as the problem is in the family”.
Key point: You can tackle the neurobiological level by medicating him. You can tackle the individual level by therapizing him. But until the problem (the family network) is addressed, the pathology will continue to flow. A strictly neurobiological formulation really misses the forest for the trees…
As a rule of thumb: neurobiological dysfunction is within the purview of psychiatric providers, individual dysfunction within the therapists domain, family level dysfunction with the family therapists domain. So fixing the individual network takes a competent therapist5. Fixing the familial network takes a competent family therapist. Fixing the societal network takes… no one has a clue. Where I see the mental-health-system fail is that it often doesn’t take this big picture view. I keep getting told that there’s a desperate shortage of psychiatric providers. I believe this is true, but I would argue the more urgent problem is that there’s a misallocation of psychiatric providers.
Let’s look at one more problem through the network lens, addiction. Below is a possible network diagram for an alcoholic. Red = significant dysfunction, orange = moderate dysfunction, and yellow = mild dysfunction.
So what we see here is that there is significant/primary dysfunction at the individual/family level, which trickles down to the neurobiological level. Alcoholics use alcohol to medicate the trickle-down-problem at the neurobiological level. This works… but for a short period of time. The problem with the alcohol-solution is that intoxication causes the individual to not fix (or actively add to) dysfunction at the source (the individual/family network).
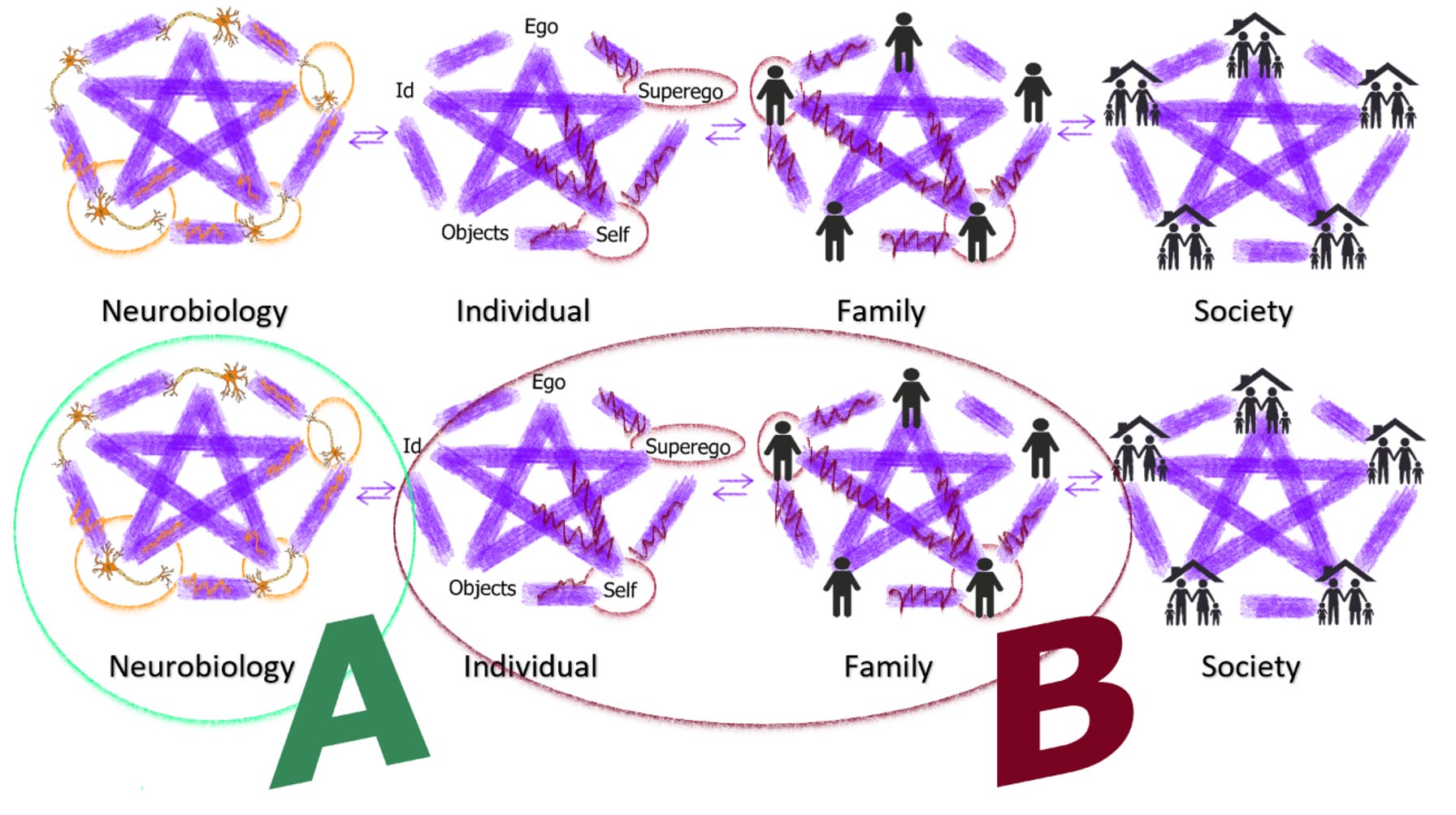
So said again: Alcohol can be viewed as temporarily mitigating the individual’s suffering at the neurobiological level (A in the figure above), with intoxication preventing them from fixing the problems at the individual/family level (B in the figure above). This is where neurobiological interpretations miss the mark. Until the addict addresses the dysfunction in B, they’re going to continue to turn to alcohol. This should make it clear why Alcoholic Anonymous is effective: it provides tools to fix the problems in the social network and the individual network. It address the core problems of a lot of alcoholics. A related situation is Borderline Personality Disorder6.
The network model shows how 2 people with the exact same disorder-phenotype can require entirely different treatments. Primary biological depression looks incredibly different from personality-disorder-depression, looks incredibly different from family-dysfunction-depression. There can exist “prototypical” versions of a disorder (and prototypical ways of drawing the network diagrams), but the variation is endless. This way of thinking applies to even the most “biological” disorders7, and emphasizes the importance of multi-modal approaches of treatment.
Implications
I don’t think this is a novel way of viewing things, but it does run counter to the paradigm that is popular today. And it isn’t just metaphysical mumbo-jumbo… mental-health viewed this way provides tangible structure to where law-makers should put their energy, and how providers use their words.
Some key take-aways and implications:
This presents a way of understanding how a disorder can have neurobiological correlates without the core deficit (and thus treatment) being neurobiological.
It emphasizes the importance of providers having a strong network of referrals to provide to patients for treatments outside the provider’s wheelhouse.
It demands a certain way of using/presenting medications in a lot of situations (“this medication might help you to get to a place to fix your problem”).
It emphasizes the importance of providers encouraging their patients to participate in social networks (“Have you been going to Church?”).
It emphasizes increasing funding towards training good therapists in different modalities (behavioral, psychoanalytic, family).
It emphasizes the need for more specialty clinics that provide treatments across multiple modalities addressing a single diagnosis (e.g. the DBT model: psychiatric provider medicates, group therapy to learn skills, individual/family therapy).
Remember, life is a magical thing because it’s so mystically complex. Acknowledging that mental health contains this complexity means that we lose our confidence in simple answers. But it also brings the magic back.

Did you know that there are cheap ways to fix this network? In addiction, instead of using the BDNF-purple-chalk, people use the DeltaFosB-shitty-pink-chalk.

You can see that drugs, sex, food, etc, fill the network with pink chalk. But as you can see from the satanic pentagram, the pink chalk is a deal with the devil. The pink chalk doesn’t last long, and when it wears off, the star is even worse off.
I can probably capture the entirety of a lot of provider’s formulation of this model on the big 3 psychiatric disorders in <30 words: For depression: Serotonin is responsible for happiness, dopamine is pleasure/motivation, norepinephrine is energy (and pain, sometimes). Schizophrenia is a dopamine deficiency (largely disregard the dopamine theory from depression). Bipolar also has something to do with dopamine, maybe, but requires “mood stabilizers” (whatever it is that they do).
I arbitrarily chose the # and name of networks so that the concept could be grasped. Technically I could go further to the left with “Receptors”, or could create more divisions in between. Also I chose psychodynamic to represent the individual based on my own preferences, but really a bazillions things could’ve been put there.
I don’t want this to get taken too far though and for this idea to get misrepresented as saying the lower levels can’t function unless the higher levels are functioning (and thus pushing a focus on societal change). I think Winnicott’s “good-enough parent” will provide a helpful analogue here.
when there is good enough mothering and good enough parentage, the majority of infants do achieve health and a capacity to leave magical control and destruction aside, and to enjoy the aggression that is in them alongside the gratifications, and alongside all the tender relationships and the inner personal riches that go to make up the life of child-hood.
D.W. Winnicott, The Child, The Family And The Outside World
I think this reasoning can be applied to every level. As an example,
when there is a good enough society, the majority of families do achieve health and a capacity…
when there is a good enough family, the majority of individuals do achieve health and a capacity…
when there is a good enough psychic health, the majority of individual’s neurobiology do achieve health and a capacity…
As a tangent, I think one way you could conceptualize the different therapies as focusing on different parts that have resonance when all worked on together, creating the star.

This is why I’m always weary of therapists who describe their approach as "eclectic". You can’t just intermingle different elements willy-nilly. Seeing 20-year-old therapists list 20 different modalities as their specialty is like watching someone who is bad at tic-tac-toe telling you that the game they like to play is 5D chess.
Here is a potential model of the dysfunction in borderline personality disorder.

Core deficits: no sense of self, distress tolerance —> ego-fragmentation, impaired object relations, problematic family dynamics. Even if the neurobiological deficits were able to be magically fixed (Abilify?, Lamictal?, Xanax? LOL), the dysfunction in the individual/family networks would still be raging. The important take-away is not that they don’t need psychopharmacological treatments, but that it’s not sufficient. A patient with borderline pathology being prescribed medication shouldn’t be told “this medication will treat your symptoms”, but rather “this medication will allow you to address the source of your problems in DBT”… and be provided with referrals to the appropriate clinics.
I think it could be argued that schizophrenia is one of the most “biological” mental health disorders. Recall that if 1 identical twins has schizophrenia, the other only has a 50% chance. Within the diagnosis, family and societal inventions are severely lacking. A lot of interventions in schizophrenia lie outside of neurobiology (Family Network: trauma, expressed emotion, Societal Network: urban life, marijuana mores).
As a person who likes network sciences, hope that this method gets more attention. What are your stances on:
1. The Braverman Test on Neurotransmitters vs Personality vs Mental Illness?
2. Associating this model with HEXACO and Schwartz/Haidt Moral Value Trends?
3. Cross-examine these value in the context of different cultural dimensions?
4. Mental Health correlation with genomic research?
You have successfully written down what I have planned to try to write down for over a year, but haven't had quite enough experience or know-how to confidently say. Kudos! One thing - Substack has an actual footnote button that autolinks to the footnote. Convenient for readers.